 nursIT Editorial Team
nursIT Editorial Team
1 min read
nursIT at Arab Health 2024
The NursIT Institute is excited to be represented at the prestigious Arab Health Exhibition 2024 in Dubai. Our managing directors, Stoyan Halkaliev...

Nursing informatics is still rarely structurally anchored in Germany. At the same time, digital applications in nursing are rapidly gaining in importance - from electronic patient records and AI-supported documentation to interoperable platforms and cross-sector care processes.
At the same time, it is becoming increasingly clear that there is a lack of qualified specialists who can combine nursing practice, IT and organization. This deficit is increasingly becoming a structural obstacle to the implementation of political, technological and organizational projects in the healthcare sector.
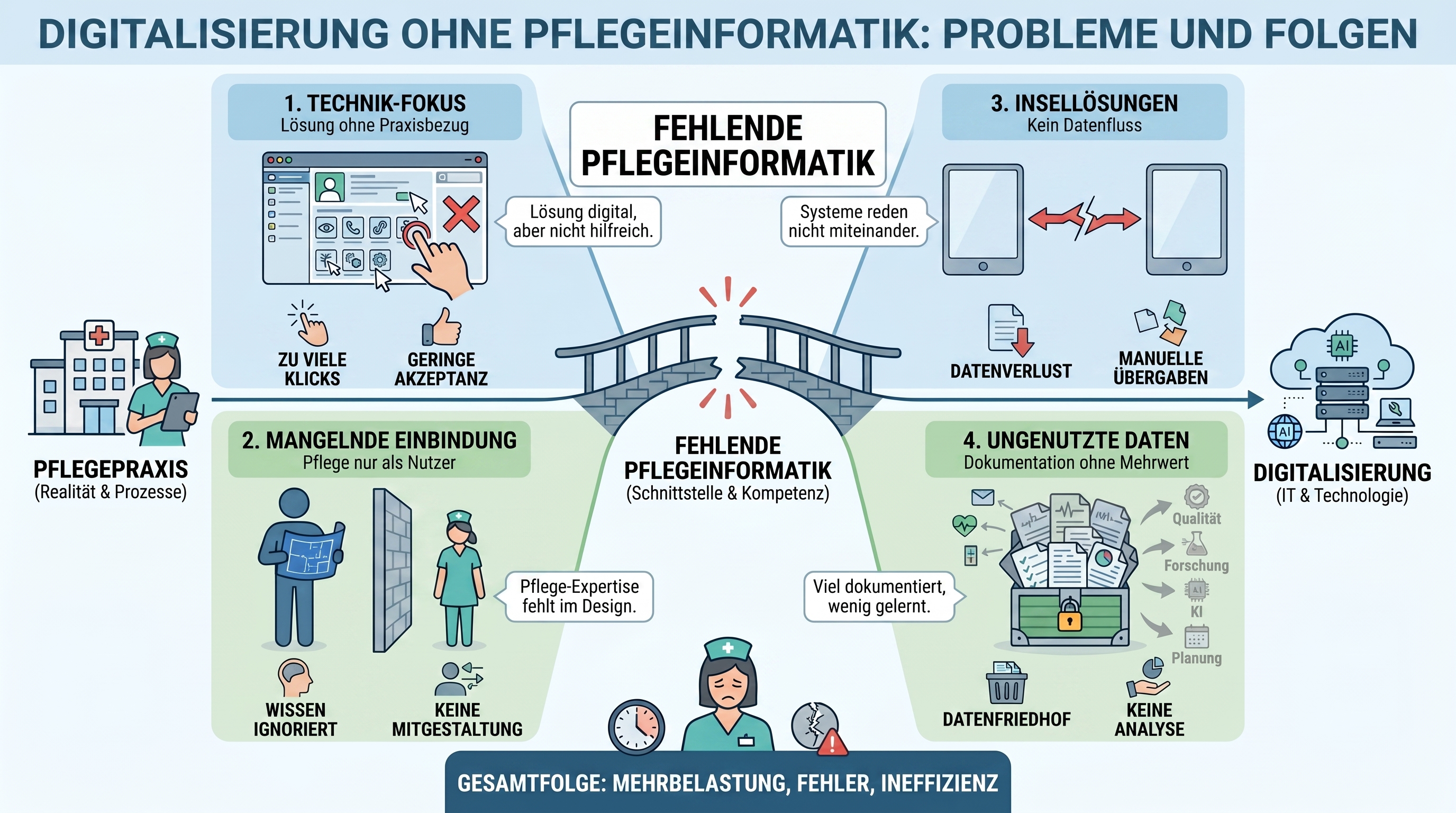
The consequences have long been noticeable in everyday nursing care: digital solutions are often introduced technically, but are not sufficiently designed in terms of nursing care. Systems then only fit real workflows to a limited extent, documentation remains time-consuming or duplicated, interfaces are missing, care data is hardly ever reused and AI applications cannot be reliably evaluated. This creates a gap between digital strategy and practical care - with the risk that digitalization creates more workload instead of relieving the burden on nursing staff and improving the quality of care.
How important is nursing informatics today - and what role must it play in the future?
This was the topic of the DMEA expert panel "Nursing informatics in Germany - insignificant or more important than ever?", organized by the German Association of Healthcare IT - bvitg e. V. and moderated by Heiko Mania, Managing Director of nursIT Institute GmbH and member of the bvitg board.
Nursing informatics does not mean that nursing staff set up printers, reset passwords or write software tickets on the side. It describes a professional interface between nursing practice, nursing science, IT, information processing and organizational development.
Heiko Mania framed the discussion from a dual perspective: from nursing practice and from health IT. As a trained nurse who has been working at the interface of nursing and digitalization for many years, he described a gap that has long accompanied Germany: While nursing care is to be increasingly digitally transformed, in many places there is a lack of people and structures that can shape this transformation in terms of nursing care.
In Germany, there are not enough established structures for nursing informatics, neither in nursing training nor in the facilities. And this is happening at a time when care is set to become more digital, data-based and increasingly AI-supported.
This is the contradiction around which the entire discussion revolved: care is to be digitally transformed, but the necessary profession has not yet been systematically established in many places.
Digitalization does not come about by purchasing systems, ordering interfaces and activating applications. It only comes about when people in the facilities understand which processes are being changed, which data is relevant, which professional groups are affected and what impact a digital solution actually has in everyday life.
Katrin Staffler, Member of the German Bundestag and Federal Government Commissioner for Nursing, had a clear message: nursing informatics must not simply be subsumed into general health or medical informatics. Nursing is not medicine. Nursing has its own processes, its own data, its own care logic and its own requirements.
Anyone who is serious about digitalization in nursing must therefore recognize nursing informatics as an independent profession.
Dr. Anika Heimann-Steinert, Product Manager at gematik, showed just how big this task is. From gematik's point of view, nursing care is not just some downstream user group, but one of the central players in the digital healthcare infrastructure.
In terms of numbers alone, this is obvious: over 30,000 outpatient and inpatient care facilities and around 1,800 clinics and hospitals are facing new challenges in the context of digital infrastructure.
But the importance of care is not just quantitative. In the provision of care, nursing is often located exactly where information should converge: between hospitals, doctors' practices, pharmacies, care facilities, relatives and patients.
This is precisely why the connection of nursing care to the telematics infrastructure is so relevant. Heimann-Steinert described how many care facilities have now set out on this path. Around 84 percent of care facilities have taken their first steps towards TI, around 60 percent can already be found in the directory service and around 40 percent have a KIM address.
These figures show progress. However, they also show that there is still a gap between formal connection and actual use. Access cards, directory service entries and KIM addresses are important steps. But they are no substitute for professional integration into the care process.
This also shows that infrastructure is necessary, but not sufficient. Without nursing IT expertise, digitization quickly becomes technically correct, but remains incomplete in practice.
The discussion became particularly concrete with Katharina Steinhauer, Chief Nursing Information Officer at Frankfurt University Hospital. Her role represents a model that is still rare in Germany: explicit nursing responsibility for digital structures, data, processes and innovations.
Steinhauer made it clear that nursing informatics should not be thought of solely in terms of the hospital information system. Nursing is more than just documentation. It includes observation, assessment, relationship, coordination, intervention, evaluation and responsibility across sector boundaries.
Your task is therefore not just to introduce digital systems. It is about formulating requirements from the care sector, testing innovations in real everyday ward life and translating them between care, IT, management and manufacturers.
Steinhauer rejected the often-heard accusation that nursing is "unwieldy" when it comes to digitalization based on her everyday experience: "If a solution has "hands and feet", it will be accepted. Scepticism arises where digitalization creates additional work instead of bringing real relief.
This is a crucial observation. Nursing staff are not hostile to digitalization. They have practical experience. And that's precisely why they recognize very quickly whether a digital system helps or just creates new click paths.
Mareike Przysucha, research assistant in the "Informatics in Healthcare" research group at Osnabrück University of Applied Sciences, brought in a scientific perspective. She focused on documentation - not as a compulsory exercise, but as an information process.
Nursing informatics not only asks: How do we document digitally? It asks: How do we turn nursing data into information, information into knowledge and knowledge into better care?
This is a fundamental difference.
Digital documentation must not mean that analog bureaucracy is simply transferred to screens. Its benefits only arise when information is recorded once, used multiple times and can be evaluated from a care perspective. When duplicate and triple documentation disappears. When care planning is supported. When risks become visible earlier. When data does not disappear into the system, but flows back into the care process.
Przysucha gave an illustrative example of this: sensor technology, such as an intelligent mattress, can recognize stress patterns and provide indications of a risk of pressure ulcers. If care can act in good time, a digital signal becomes concrete prevention. Digitalization is then not an end in itself, but better care.
Hardly any other topic is currently shaping healthcare IT as much as artificial intelligence. Expectations are also high in the care sector: AI should make documentation easier, structure texts, identify risks, support care planning and reduce routine activities.
However, the panel discussion also showed the other side: AI increases the need for expertise.
Anyone using AI in care must understand what such systems do, what data they use, where their limits lie and how results can be classified responsibly. Particularly in the context of the EU AI Act, it is clear that facilities need employees who can not only operate AI, but also understand it professionally and organizationally.
This makes care informatics a prerequisite for responsible AI in care. Without it, there is a risk that AI solutions will be sold as promises but not sufficiently tested, evaluated and translated into the reality of care.
A contribution from the audience brought the discussion to a very specific area: the digital care transition form.
The question was: Why is the digital doctor's letter taken for granted, while the care transfer form is still not available across the board in 2026?
Dr. Heimann-Steinert reminded the audience that the PIO transition sheet has already been specified. So the problem is not that there is no technical basis. The problem lies in prioritization, complexity, financing and commitment.
Care transition is challenging because it combines different sectors, facilities, documentation logics and nursing content. But that is precisely why it is so important. If care information is missing at transitions, gaps in care arise. And if nursing data is not given the same digital status as medical documents, nursing care remains structurally underrepresented.
In addition, other digital information objects have been prioritized more strongly, even where European requirements such as the EHDS create additional pressure. For the care transition form, this means that although the specification is available, there is no binding implementation push.
Heimann-Steinert described it matter-of-factly: without a commitment, many things will only be implemented on an "as needed" basis. And in practice, "as needed" often means that the customer pays.
The care transfer sheet is therefore more than an isolated case. It is a symbol for the question of what place care actually has in the digital healthcare infrastructure.
A particularly critical point of the discussion was the lack of a training structure. Mareike Przysucha made it clear that Germany first needs a common vision: What should nursing informatics specialists be able to do? What roles do they take on? Where do they work? What skills do they need?
We need a common vision of "where we actually want to go", saidPrzysucha. Without such a target image, individual initiatives will get underway, but not necessarily in the same direction.
Although there are currently e-health and health informatics offerings, there are hardly any explicit, permanently established study or further education paths for nursing informatics. Many initiatives were project-dependent. When the funding ends, the offer often ends too.
That is not enough.
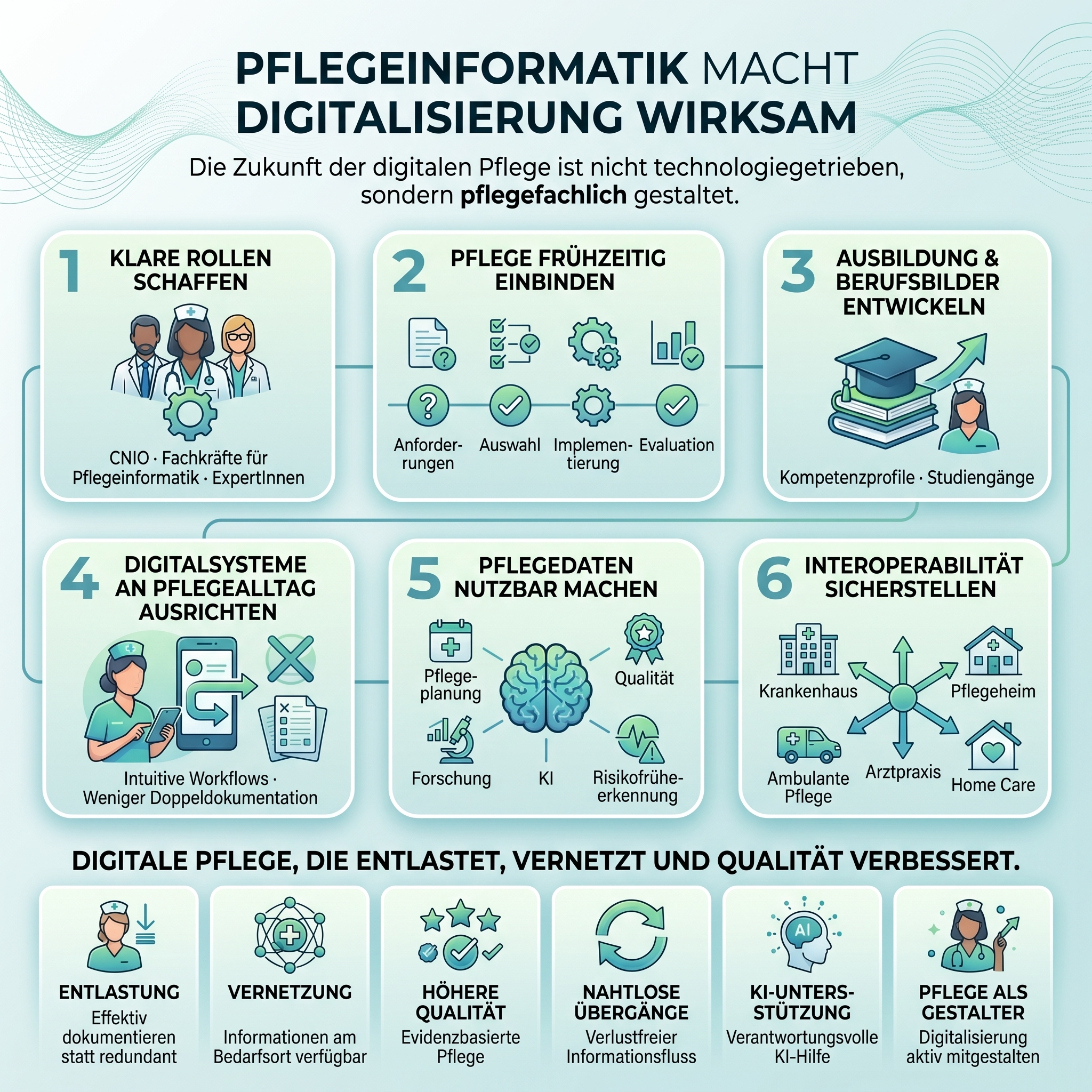
Nursing informatics needs a clear job description, binding skills profiles, study programs, further training opportunities and career paths in institutions. Otherwise it will remain dependent on individuals, coincidences and local special paths.
This is precisely one of the biggest tasks for politicians, universities, associations and institutions.
In the end, Heiko Mania condensed the discussion into a central statement: it is no longer a question of whether the healthcare system can afford nursing informatics. The real question is whether it can afford to plan, document and make decisions without nursing informatics.
That is the core issue.
Because digitalization without nursing informatics means that systems are introduced without sufficiently understanding nursing processes. Data is collected without ensuring that it is useful for nursing care. AI is discussed without establishing competence structures. Interoperability is demanded without consistently considering nursing content. Nursing staff are involved but not always empowered to help shape digital transformation themselves.
Nursing informatics is therefore not a special topic for particularly tech-savvy nursing staff. It is a strategic prerequisite for modern care.
The discussion at the DMEA made it clear that nursing informatics is no longer on the fringes of the digitization debate in Germany. It belongs at its center.
The technical possibilities are there. The political digitization goals have been formulated. The necessity is obvious. What is missing is the systematic anchoring of a profession that really thinks about care, technology and data together.
Nursing informatics must therefore be integrated into training, further education, universities, institutions, funding programs, product development, research and political strategies.
Not as an additional task. Not as a secondary role. But as an independent competence for care that is becoming more digital - and must improve in the process.
Because in the end, the success of digitalization is not determined by the question of whether a system works technically. Rather, it depends on whether it improves care, relieves the burden on care and benefits people.
This is precisely where nursIT's perspective lies. Since our foundation, we have been working at the interface of care practice, health IT and digital process design. Our solutions are not developed from a purely technical view of the hospital, but from an understanding of nursing reality: How do people work on the ward? What information is really needed? Where do media breaks occur? Which documentation is helpful - and which is a burden?
This proximity to nursing is one of our key strengths. nursIT combines nursing process knowledge with interoperable technology, digital documentation and the experience gained from numerous projects in hospitals and care structures. This puts us right at the interface that was discussed in the expert panel: between nursing, IT, organization and care practice.
We would like to thank all the participants in the expert panel for their professional input, their different perspectives and the open discussion. We would also like to thank the Bundesverband Gesundheits-IT - bvitg e. V. for organizing the session and the DMEA for providing the framework to make this important topic visible.
Moderation
Heiko Mania
Member of the board at Bundesverband Gesundheits-IT - bvitg e. V.
Speaker
Dr. Anika Heimann-Steinert
Product Manager at gematik GmbH
Mareike Przysucha
Research assistant in the research group "Informatics in Healthcare" at Osnabrück University of Applied Sciences
Katrin Staffler, Member of the Bundestag
Federal Government Commissioner for Nursing Care at the Office of the Federal Government Commissioner for Nursing Care
Katharina Steinhauer
Chief Nursing Information Officer at University Medicine Frankfurt / Nursing IT & Innovation Unit

1 min read
The NursIT Institute is excited to be represented at the prestigious Arab Health Exhibition 2024 in Dubai. Our managing directors, Stoyan Halkaliev...

1 min read
From our previous market research trips to France, we know that FHIR® 🔥 will also play a crucial role in the digitalization strategies of hospitals...

1 min read
On November 9th, a transformative event took place: The smartXcare 2023 at the Karl Storz Visitor and Training Center in Berlin. This gathering...